
Grantee Research Project Results
2015 Progress Report: Endotoxin Exposure and Asthma in Children
EPA Grant Number: R834515C001Subproject: this is subproject number 001 , established and managed by the Center Director under grant R834515
(EPA does not fund or establish subprojects; EPA awards and manages the overall grant for this center).
Center: Denver Childrens Environmental Health Center - Environmental Determinants of Airway Disease in Children
Center Director: Guo, Yanbing
Title: Endotoxin Exposure and Asthma in Children
Investigators: Schwartz, David A. , Covar, Ronina A , Litonjua, Augusto A. , Liu, Andrew H. , Crooks, James L , Van Dyke, Michael V. , Forssen, Anna , Sordillo, Joanne , Rabinovitch, Nathan , Szefler, Stanley , Fingerlin, Tasha
Institution: National Jewish Health , Harvard University , National Jewish Medical and Research Center
EPA Project Officer: Hahn, Intaek
Project Period: June 22, 2010 through June 21, 2015 (Extended to June 21, 2017)
Project Period Covered by this Report: June 22, 2015 through June 21,2016
RFA: Children's Environmental Health and Disease Prevention Research Centers (with NIEHS) (2009) RFA Text | Recipients Lists
Research Category: Children's Health , Human Health
Objective:
We hypothesize that higher levels of endotoxin exposure cause persistent, problematic asthma and that key environmental (ozone and allergens) and genetic modifiers (endotoxin receptor polymorphisms) contribute to endotoxin susceptibility and pathological asthmatic responses. We are studying these endotoxin-induced airway conditions in children through three complementary clinical investigations.
First, we are capitalizing on an ancillary study of a NIH-sponsored multi-center cohort of children with asthma (Childhood Asthma Management Program), which has tracked asthma severity for over a decade, to determine if endotoxin exposure, modified by genetics and environment, is associated with greater disease severity and persistence.
Second, we have planned a panel study of children with asthma to investigate whether endotoxin exposure, modified by environment, is associated with inflamed airways and elevated toll-like receptor (TLR) expression on airway macrophages. Clinically, these inflammatory responses could drive poor asthma control and exacerbations.
Finally, we have taken advantage of a Department of Housing and Urban Development (HUD)-sponsored inner city home intervention study to determine if a home environment intervention will reduce home endotoxin levels and improve asthma. This combination of studies is expected to provide an understanding of how endotoxin interacts with other potentially toxic exposures in the susceptible host to cause persistent, problematic asthma. These studies will help us to determine the levels of endotoxin exposure that are likely to be problematic for children with asthma, and to develop environmental educational and intervention programs to improve health outcomes.
Progress Summary:
As proposed, three complementary studies address the aims and hypotheses of Project 1: (1) Childhood Asthma Management Program (CAMP) ancillary study; (2) Denver Asthma Panel Study (DAPS); and (3) Housing & Urban Development (HUD) ancillary study. Based on our Center's research experience, progress and findings so far, we sought to strengthen the accuracy and relevance of our exposure assessments in DAPS by adding personal wearable exposure monitoring and bedroom air stationary monitoring. With EPA approval in January 2014, we successfully added and completed our Endotoxin Personal Exposure Monitoring Study (EPEM) to enhance, operationalize and validate personal exposure monitoring for the longitudinal DAPS. Until recently, the lab assay for endotoxin has utilized limulus amebocyte lysate, a reagent that cross-reacts with molds. Now, there is an endotoxin assay based on recombinant Factor C (rFC), which only binds with endotoxin. To advance scientific understanding of pure endotoxin exposure (i.e., independent of mold) and asthma outcomes, we developed and validated a Standard Operating Procedure to measure endotoxin using the rFC assay, and established quality control parameters.
(1) Our CAMP investigation is the first study, to our knowledge, to clearly distinguish household endotoxin from mold exposure in children with asthma. By using the endotoxin-specific rFC assay and separate mold exposure measures (i.e., mold plate counts), we evaluated the effects of household endotoxin and mold exposures on asthma severity. In fact, we found that higher endotoxin levels in baseline dust samples (n = 962) were associated with fewer prednisone days (an indicator of severe asthma exacerbations), while high mold counts were associated with more prednisone days during the 4-year course of the study. Only weak correlations were found between log mold concentrations and endotoxin levels (unadjusted r = 0.17; p = < 0.0001). When the effects of endotoxin and mold exposures on prednisone days were assessed for each site (with both exposures in the model), endotoxin-associated reductions and mold-associated increases in prednisone days were found for 5 of the 8 CAMP sites (Baltimore, Denver, San Diego, St. Louis, and Toronto), consistent with the overall model.
We also investigated the interaction of endotoxin with 48 SNPs in 11 Toll-Like Receptor (TLR) genes (TLR-1, -2, - 3, -4, -5, -6, -9, -10, CD14, MyD88, LY96, ACAA1) on severe asthma exacerbations (i.e., at least one ER visit or hospitalization for asthma in the past year). This preliminary analysis was restricted to CAMP participants of Caucasian ethnicity: 517 CAMP Caucasian participants included 84 cases with at least one severe asthma exacerbation vs. 433 controls. For two single nucleotide polymorphisms (SNPs) (in TLR9 and MyD88), the presence of the dominant genotype and higher endotoxin levels increase the risk of severe asthma exacerbations. Because of these significant TLR geneendotoxin interactions, we expanded our genotyping of genes downstream of the TLR receptor complex. We also performed a genome-wide, pathway level analysis to develop a gene-by-environment model for endotoxin exposure and asthma exacerbations. Glycosphingolipid metabolism showed the most evidence for interaction with endotoxin exposure at the pathway level in models of asthma severity. Endotoxin interactions with gene polymorphisms in SPTLC2, ASAH1, GALC, ARSB, PPAP2B and SPTLC1 contributed to glycosphingolipid pathway enrichment. Other pathways and functional groupings that showed possible interactions with environmental endotoxin included muscarinic and histamine receptors, the nitric oxide synthase pathway, and Fc Epsilon Receptor 1 signaling in mast cells. Pathway level analysis identified functional groupings of genes that may interact with ambient endotoxin exposure to alter asthma severity in children. These gene-by-environment interactions would not have been detected in a conventional genome wide survey of individual SNP-level gene-by-environment associations.
(2) For DAPS, we strengthened the accuracy and relevance of our exposure assessments by adding personal wearable exposure monitoring and bedroom air stationary monitoring. With EPA approval in January 2014, we successfully added and completed the Endotoxin Personal Exposure Monitoring study (EPEM) to develop, enhance, and operationalize personal exposure monitoring methods for DAPS. The DAPS protocol was developed to include these exposure monitoring enhancements and received IRB approval, and participant enrollment began in July 2014. Study participant enrollment was recently completed (n = 56). Currently, 13 have completed the study (87% retention) and the remainder are continuing and on target for study completion within the funding period.
Preliminary analyses were performed to validate exposure monitoring methods using the first study visit data from these early DAPS enrollees and additional EPEM study participants with asthma meeting DAPS criteria (n = 25). Clinical measures of asthma severity (spirometry, exhaled nitric oxide, and Composite Asthma Severity Index (CASI)) were assessed concurrent with deployment of monitors.
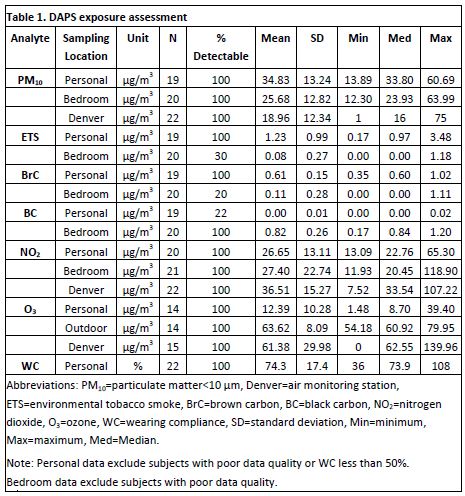
Exposure Samplers: The wearable Microminiature Personal Exposure Monitor (MicroPEM™, RTI International) and stationary Personal Environmental Monitor (PEM™, MSP Corp) samplers were used to measure particulate matter < 10 μm (PM10) via gravimetric analysis and real-time nephelometry as well as components of PM10 – including black carbon (BC), brown carbon (BrC), and environmental tobacco smoke (ETS) – via spectrophotometry. Ogawa™ passive badges (Ogawa USA) were used to measure O3 and NO2. Publicly available Air Quality Index (AQI) data, from a Colorado Department of Public Health (CDPHE) air monitoring station in central Denver, were used for outdoor (ambient) comparisons of PM10, NO2, and O3. Table 1 presents summary statistics for exposure assessments.
Exposure Monitor Deployment and Clinical Asthma Severity Assessments: Ogawa™ passive badges and PEM™ monitors were installed in participants’ bedrooms. Ogawa™ passive badges were also installed outside of the home during the summer visit. Each participant was fitted with a personal monitoring apparatus (MicroPEM™, Ogawa™ passive badges, and iTrack Micro™ GPS device). All devices were retrieved after approximately 72 hours. Spirometry, exhaled nitric oxide (eNO), and Composite Asthma Severity Index (CASI) [Wildfire JJ et al (Liu AH co-author). J Allergy Clin Immunol. 2012; PubMed PMID: 22244599] were assessed concurrent with deployment of monitors and badges.
Feasibility of exposure assessment using wearable monitors in children. Wearing compliance (WC) was calculated from MicroPEM™ accelerometry data and the personal exposure log. Statistical analyses included participants with greater than 50% (“acceptable”) wearing compliance based on thresholds used in prior studies. WC was acceptable in 91% of participants, with a median WC of 78% for those with acceptable WC.
Environmental exposures are detectable and correlate with clinical assessments. Personal versus stationary exposures were analyzed with linear mixed models or Wilcoxon signed rank tests depending on the statistical distributions. Personal exposure levels were significantly higher than stationary bedroom levels for PM10 (p = 0.025), BrC (p = 0.0005), and ETS (p < 0.0001). In contrast, personal levels for BC were significantly lower than stationary bedroom levels (p < 0.0001). Linear regression models assessed how pollutant levels were associated with asthma severity, and were adjusted for age, race and gender, when applicable. Linear regression analyses revealed multiple significant exposure-asthma severity correlations (Table 2). Personal exposure-asthma severity correlations were stronger than stationary exposure-asthma severity correlations, suggesting that personal monitors provide more accurate measurements of environmental exposures.
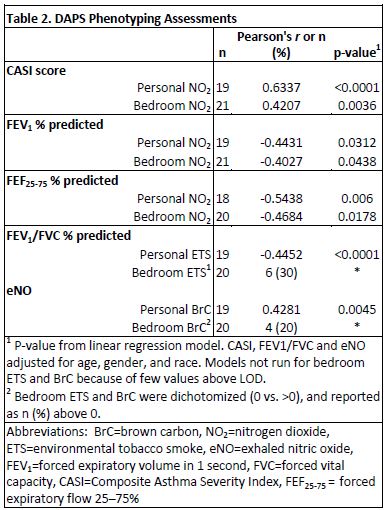
Personal monitoring with the MicroPEM has been validated as better than stationary monitoring for some exposures. Preliminary DAPS analyses have shown that personal monitors measure NO2 more accurately, and provide better detection of ETS and BrC. As a result, the personal monitors reveal correlations between asthma severity and air pollutant exposures that are missed by conventional stationary monitors. Similarly, in a prior collaboration with RTI, research with backpack personal monitors demonstrated better endotoxin-asthma severity correlations than did stationary monitors. Greater exposure to personal endotoxin (1 EU/m3 change) was associated with more asthma symptoms during sleep (p = 0.04) and lower FEV1 (p = 0.04; correlation p = 0.15), but exposure to indoor stationary endotoxin was not significant [Rabinovitch N, Liu AH, et al. J Allergy Clin Immunol. 2005; PubMed PMID: 16275375]. Personal monitoring has not yet been validated for allergens, glucans (molds), black carbon, or O3 with respect to exposure-asthma severity correlations. Therefore, we will continue to use standard methods, stationary air filters and dust sample collection, in addition to personal monitoring.
Collaborations have been established. DAPS substudies have helped to develop and strengthen collaborative relationships for DAPS by piloting some of the proposed research with the investigators and exposure monitoring group involved in this study: Andrew Liu (Project 1 Leader and DAPS research team), Jonathan Thornburg (RTI International), and James Crooks (Biostatistician and Environmental Epidemiologist, NJH). These preliminary analyses have shown that personal monitors measure respirable pollutant exposures more accurately. As a result, the personal monitors reveal correlations between asthma severity and air pollutant exposures that are missed by conventional stationary monitors. These enhanced exposure monitoring methods have been incorporated into the DAPS study. These findings were selected for presentation at the 2015 American Academy of Allergy, Asthma & Immunology Annual Meeting (Best of Environmental and Occupational Respiratory Diseases Interest Section) and the 2015 American Thoracic Society International Conference, and are being developed for publication.
(3) For the HUD study, 115 participants were enrolled, and the study participant follow-up visits were completed in March 2012. The HUD cohort comprised mostly ethnic minority children, with asthma, living in low-income housing. The homes had many asthma triggers that were targets for remediation at three levels: Education Only, Minor Remediation, and Moderate Remediation. All families received an educational intervention consisting of results from their home environmental assessment and tailored educational materials and remediation recommendations based on these results, such as EPA’s publications: Clear Your Home of Asthma Triggers; A Brief Guide to Mold, Moisture, and Your Home; and Protect Your Family and Yourself from Carbon Monoxide. All families with a smoker living in the house received guidance on establishing a smoke-free home and referral to the Colorado QuitLine, a free phone-based smoking cessation program. Endotoxin concentration was measured in 262 house dust samples collected from the general living area and participant’s bedroom. Seventy homes had all dust samples collected, meaning adequate dust samples for endotoxin measurement from both general living area and bedroom, before (Pre) and 6 months after (Post) remediation. Remediation did not significantly reduce house dust endotoxin levels measured 6 months later (Wilcoxon Rank Sums test).
Future Activities:
The coming, final year will include continuation of DAPS visits to completion of the DAPS study, and analyses and preparation of our findings for presentation and manuscript submissions. We completed our collaborative investigation of endotoxin exposure and asthma outcomes in 150 inner city children in Baltimore and a manuscript of our findings was published. We also completed a collaborative investigation of endotoxin exposure and early childhood wheezing phenotypes in a Denver inner city pre-school cohort. What we have learned from our CAMP, EPEM, MAACS, HUD and CAPS studies, and the other Projects and COTC in our CEHC, has informed and strengthened DAPS.
References:
Wildfire JJ et al (Liu AH co-author). J Allergy Clin Immunol. 2012; PubMed PMID: 22244599
Rabinovitch N, Liu AH, et al. J Allergy Clin Immunol. 2005; PubMed PMID: 16275375
Journal Articles on this Report : 1 Displayed | Download in RIS Format
| Other subproject views: | All 23 publications | 14 publications in selected types | All 14 journal articles |
|---|---|---|---|
| Other center views: | All 51 publications | 30 publications in selected types | All 30 journal articles |
| Type | Citation | ||
|---|---|---|---|
|
|
Matsui EC, Hansel NN, Aloe C, Schiltz AM, Peng RD, Rabinovitch N, Ong MJ, Williams DL, Breysse PN, Diette GB, Liu AH. Indoor pollutant exposures modify the effect of airborne endotoxin on asthma in urban children. American Journal of Respiratory and Critical Care Medicine 2013;188(10):1210-1215. |
R834515 (2012) R834515 (2013) R834515 (2014) R834515 (2015) R834515 (Final) R834515C001 (2014) R834515C001 (2015) R834515C002 (2014) R834515C003 (2014) R834510 (2014) |
Exit Exit Exit |
Supplemental Keywords:
Endotoxin, exposure, children, asthma, risk, health effects, susceptibility, sensitive populations, genetic pre-disposition, genetic polymorphism, indoor air, dose-response, ozone, remediation, human health, health, health effects, biology, health risk assessment, children's health, allergens/asthma, asthma indices, intervention, Health, Scientific Discipline, HUMAN HEALTH, Health Risk Assessment, Physiology, Biology, Allergens/Asthma, Health Effects, sensitive populations, airway inflammation, asthma, asthma indices, asthma triggers, children, endotoxin, allergic responseRelevant Websites:
Research Programs and Departments | National Jewish Health ExitProgress and Final Reports:
Original AbstractMain Center Abstract and Reports:
R834515 Denver Childrens Environmental Health Center - Environmental Determinants of Airway Disease in Children Subprojects under this Center: (EPA does not fund or establish subprojects; EPA awards and manages the overall grant for this center).
R834515C001 Endotoxin Exposure and Asthma in Children
R834515C002 Environmental Determinants of Early Host Response to RSV
R834515C003 Environmental Determinants of Host Defense
The perspectives, information and conclusions conveyed in research project abstracts, progress reports, final reports, journal abstracts and journal publications convey the viewpoints of the principal investigator and may not represent the views and policies of ORD and EPA. Conclusions drawn by the principal investigators have not been reviewed by the Agency.